

How Kennedy's FDA And CDC Cuts Imperil Your Family's Health
Robert F. Kennedy, Jr. swung his meat axe at the Health and Human Services Department on Thursday, leaking plans to theWall Street Journal that he plans to lay off 10,000 workers or about 12 percent of the department’s workforce.
If he follows through on the plan, the largest layoffs will come at the Food and Drug Administration and the Centers for Disease Control and Prevention — the two sub-agencies that drew his greatest ire while running for president. The leaked plan calls for eliminating 3,500 full-time positions at FDA and 2,400 at CDC, which represents nearly 60 percent of the total employment cuts.
“If you work for the FDA and are part of this corrupt system, I have two messages for you: 1. Preserve your records, and 2. Pack your bags," Kennedy wrote on X last October after endorsing the Trump campaign.
The memo said the three divisions at FDA that approve new drugs, biologics and medical devices, which depend largely on industry user fees for their funding, would be exempt from the cuts. Those three sub-agencies employ 11,800 of the FDA’s total workforce of 19,700.
That means the bulk of the layoffs will come in the agency’s Human Food Program, which employs a little less than 8,000. Eliminating 3,500 its workers would nearly halve a sub-agency that protects the nation’s food supply; oversees food additives and dietary supplements; and crafts nutrition guidelines and food labels.
Staff who work in foods who were not exempted from the cuts include people who work on solving, communicating, and preventing outbreaks; testing foods for contaminants like heavy metals or bacteria; developing nutrition and food labeling policy; and take enforcement against companies who break the law.
Roughly two-thirds of Human Food Program funding goes towards inspection or ‘field’ personnel aimed at keeping our food supply safe, said Sarah Sorcher, director of regulatory affairs at the Center for Science in the Public Interest, in an email. (Full disclosure: I worked there from 2004-2009.) “Cuts are likely to hit heaviest on the foods program,” she said. “There are a few reviewers working on pre-market approval of additives, including food contact substances, (so) this is a very small fraction of the workforce.”
A corporate field day
No doubt the food additives regulatory function that Kennedy’s Make America Healthy Again campaign put in its crosshairs will be decimated. Eliminating workers without having an alternative regulatory scheme in place could prove disastrous for the American public.
First, the food and chemical additives industry will fight any attempt to ban or regulate their products, using its small army of lobbyists to slow the regulatory process before going to the business-friendly courts to prevent implementation. Second, the supplements industry will enjoy a field day after a sharp reduction in staff at FDA.
With fewer personnel to conduct oversight, shyster-led companies will fill the airwaves and internet with ads making unproven health claims for products that have never been tested for safety and efficacy. In addition to Kennedy’s long history questioning vaccine safety, Kennedy in recent years backed unproven medical claims such as taking cod liver oil for measles and ivermectin and hydroxychloroquine for Covid.
If the Trump administration follows through on the cuts, Dr. Martin Makary, the newly confirmed head of FDA, will be handed a shattered agency incapable of carrying out many of its core functions. During his confirmation hearing, which took place shortly after the initial Elon Musk-ordered employment cuts at the agency were rolled back, Makary promised senators he would do his own assessment of personnel needs at the agency. This latest plan raises the obvious question of whether he played any role at all in evaluating staffing.
A surgeon by training, Makary during his hearing also revealed an affinity for blaming the marginal issues championed by his new boss for the rise in childhood illness, where the main problems in recent years have been identified as rising obesity caused by junk food diets and lack of exercise, environmentally-caused asthma and the return of once-conquered childhood illnesses due to vaccine hesitancy. When asked by a MAHA-friendly senator about the role food additives play in causing inflammation and gut microbiome alterations, Makary replied, “Half of our nation's children are sick and nobody has really been doing anything meaningful on this front … We have to look at those ingredients.”
States will be hit hard by CDC cuts
The employment cuts at CDC contained in the new Trump administration plan will eliminate an estimated 19 percent of all agency jobs. Many research functions, like the reports that go into the Morbidity and Mortality Weekly Report, may fall by the wayside. Here’s the internet front page of a recent issue:
Public health agencies across the country, journalists and academic researchers rely on MMWR reports to identify emerging trends, deploy scarce resources, and identify issues that need further study. But Russell Vought, one of the key architects of Project 2025 and President Trump’s current director of the Office of Management and Budget, told Michigan’s Hillsdale College forum last September that most CDC workers “don’t even do public health. They are researchers that publish material. Who knows if it’s even relevant or not?”
Earlier this week, the administration announced it will cancel tens of billions of dollars in CDC grants to state and local health departments, which are dependent on federal funding to track infectious diseases, health disparities, vaccinations, mental health services, and other public health issues. It sent stop-work-immediately notices to the states, according to a news report in The Hill.
Many of the grants were authorized in the Covid relief bills passed during the Biden administration, which expire this September. Besides fighting the pandemic, state and local health officials used the money to also track the ongoing measles outbreak, improve their antiquated computer systems, and invest in other public health priorities.
States will soon become wholly dependent on their own resources to carry out these functions even as their residents continue to send most of their tax money to the federal government.
Merrill Goozner, the former editor of Modern Healthcare, writes about health and politics at GoozNews.substack.com, where this column first appeared. Please consider subscribing to support his work.
Reprinted with permission from Gooz News.


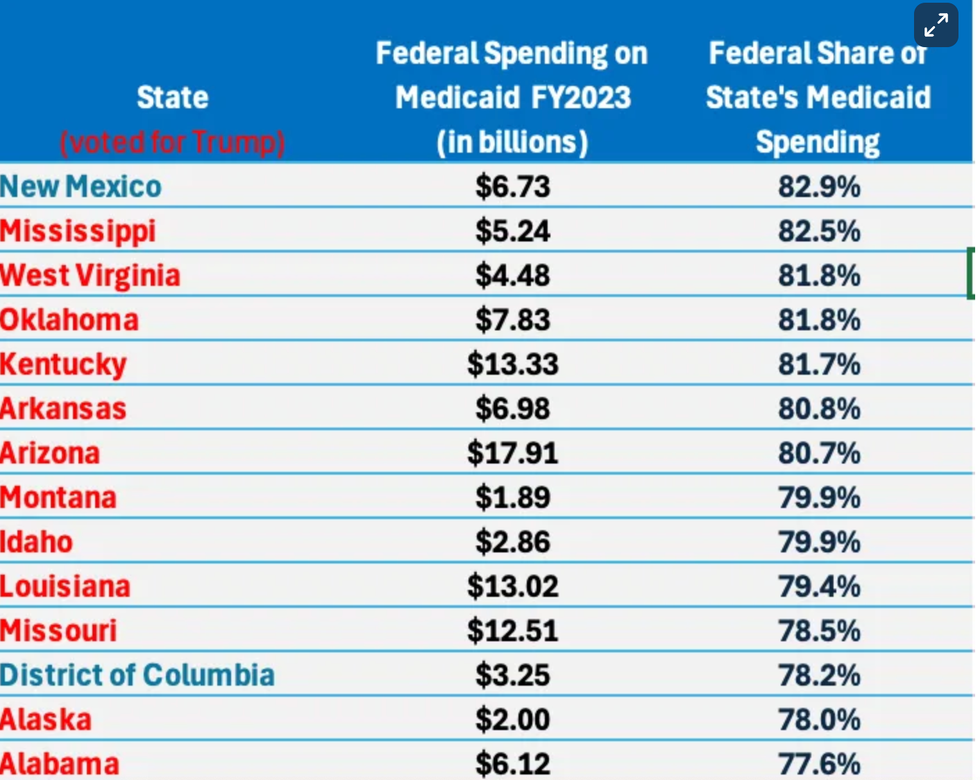 Top 14 states most reliant on federal matching funds for Medicaid
Top 14 states most reliant on federal matching funds for Medicaid

